It’s Monday a new week and I’m still resting the leg 🙄( solid resting from walking since Friday) it’s a new pain that until last week I’d never experienced before. Thankfully I’ve been able to do my yoga, which is gentle and nice, and doesn’t activate it, as it’s from stepping and lifting up to step that was causing it.
However it has made me chase up my consultant appointment filling the CT scan done in October. And by luck I grabbed someone else’s cancelled one, so it’s 22nd November I get to see them. Nervous though, and I hope I can get it across how much the lower back and now lower leg pain is affecting me.

The most common complications following hip arthroplasty are leg length discrepancy and hip dislocation. Leg length discrepancy is relatively common following hip arthroplasty, with an incidence as high as 20% to 50%.
Maintaining equal leg length intraoperatively is a challenge for orthopedic surgeons, whose goal is to ensure normal gait and hip function postoperatively. To achieve increased hip stability, the surgeon may use a larger prosthesis, which may result in increased leg length compared with the contralateral side. Leaving an extremity shortened may result in postoperative hip instability, which is far more problematic.

Preoperative assessment should include careful screening for differences in leg length, including hip contracture, pelvic obliquity, and congenital issues. Preoperative radiographs of the hip are used by orthopedic surgeons to create a template of the hip and determine the appropriate implant size. Achieving hip stability generally takes priority during surgery, and a small length discrepancy is considered acceptable in most cases.
Few patients with increased leg length will notice or have symptoms. However, large length discrepancies may cause postoperative nerve injury to the leg, gait disorders, and lower back and hip pain. A large difference in leg length is a significant source of dissatisfaction after hip arthroplasty and is one of the most common reasons for lawsuits against orthopedic surgeons.
Most people will tolerate a leg length discrepancy of up to 10 mm or approximately 3/8 inch. A difference of ≥1 cm, or approximately 7/16 inch, is noticeable in up to 50% of patients, and of those, 15% to 20% require shoe correction to resolve symptoms caused by the discrepancy.
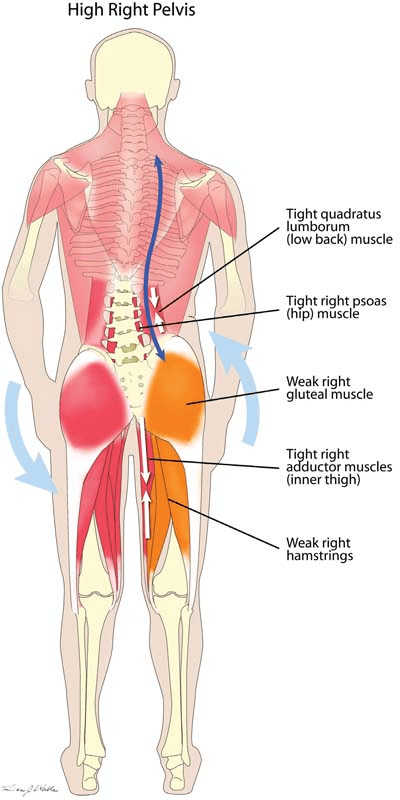
Small leg length discrepancies can be treated with heel lift shoe inserts, but a lift >3/8 inch generally does not fit well in a shoe. A discrepancy of ≥7/16 inch generally requires a lift at the shoe bottom, and a discrepancy >2 cm generally requires surgical correction, but how now when both hips are replaced? And would I risk it again? Muscle tightness, pelvic tilt, and altered gait may cause leg length discrepancies after hip arthroplasty but these issues usually self-correct within 6 months of surgery and therefore shoe lifts generally are not prescribed until after this time period. I’ve definitely given it a whole year of being proactive in physio and exercise to no avail. Time to get some real answers and map out solutions for the future.
In the meantime you’ll find me, reading books and nursing a hot water bottle on my never ending back pain.

Leave a comment